Instructions on Utilizing Ada Dental Claim
Filling out the ADA Dental Claim Form can seem daunting, but with a little guidance, you can navigate it with ease. This form is essential for submitting your dental claims to insurance companies or dental benefit plans. Each section requires specific information, and it's crucial to provide accurate details to ensure timely processing. Follow these steps to complete the form successfully.
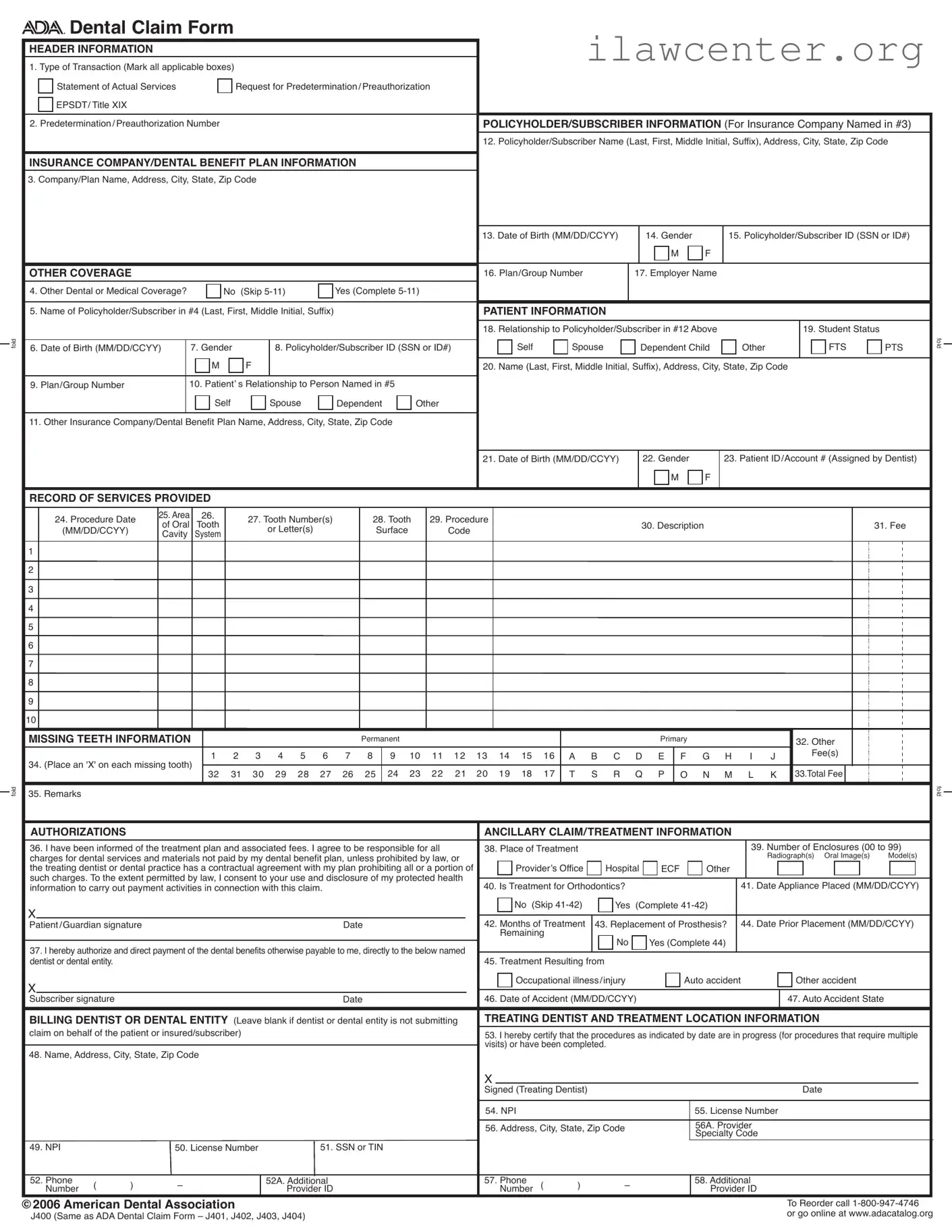
- Header Information: Mark all applicable boxes for the type of transaction at the top of the form. This includes options like "Statement of Actual Services" or "Request for Predetermination/Preauthorization."
- Policyholder/Subscriber Information: Fill in the policyholder's name (last, first, middle initial, suffix), address, city, state, and zip code.
- Insurance Company Information: Enter the name of the insurance company or dental benefit plan, along with its address, city, state, and zip code.
- Date of Birth and Gender: Provide the policyholder's date of birth (MM/DD/CCYY) and gender (M/F).
- Policyholder ID: Input the policyholder's ID number or Social Security Number (SSN).
- Other Coverage: If there is other dental or medical coverage, answer "Yes" and complete the required sections (5-11). If not, skip to the patient information section.
- Patient Information: Fill in the patient's relationship to the policyholder, their date of birth, gender, and ID/account number assigned by the dentist.
- Record of Services Provided: For each procedure, list the date, area, tooth number(s), procedure code, description, and fee.
- Missing Teeth Information: Indicate any missing teeth by placing an 'X' on the appropriate teeth.
- Authorization: Sign and date the authorization section, confirming you understand the treatment plan and associated fees.
- Treating Dentist Information: Complete the details for the treating dentist, including their name, address, and NPI.
- Billing Dentist Information: If applicable, fill in the billing dentist's information, including their NPI and phone number.
Once you have completed the form, double-check all the information for accuracy. It's essential to ensure that each section is filled out correctly to avoid delays in processing your claim. After confirming everything is correct, you can submit the form to your insurance company or dental benefit plan for review.