Instructions on Utilizing Biopsychosocial Assessment Social Work
Completing the Biopsychosocial Assessment Social Work form is an important step in your journey toward receiving the support you need. The information you provide will help professionals understand your unique situation and tailor their approach to best assist you. Please take your time to fill out each section thoughtfully.
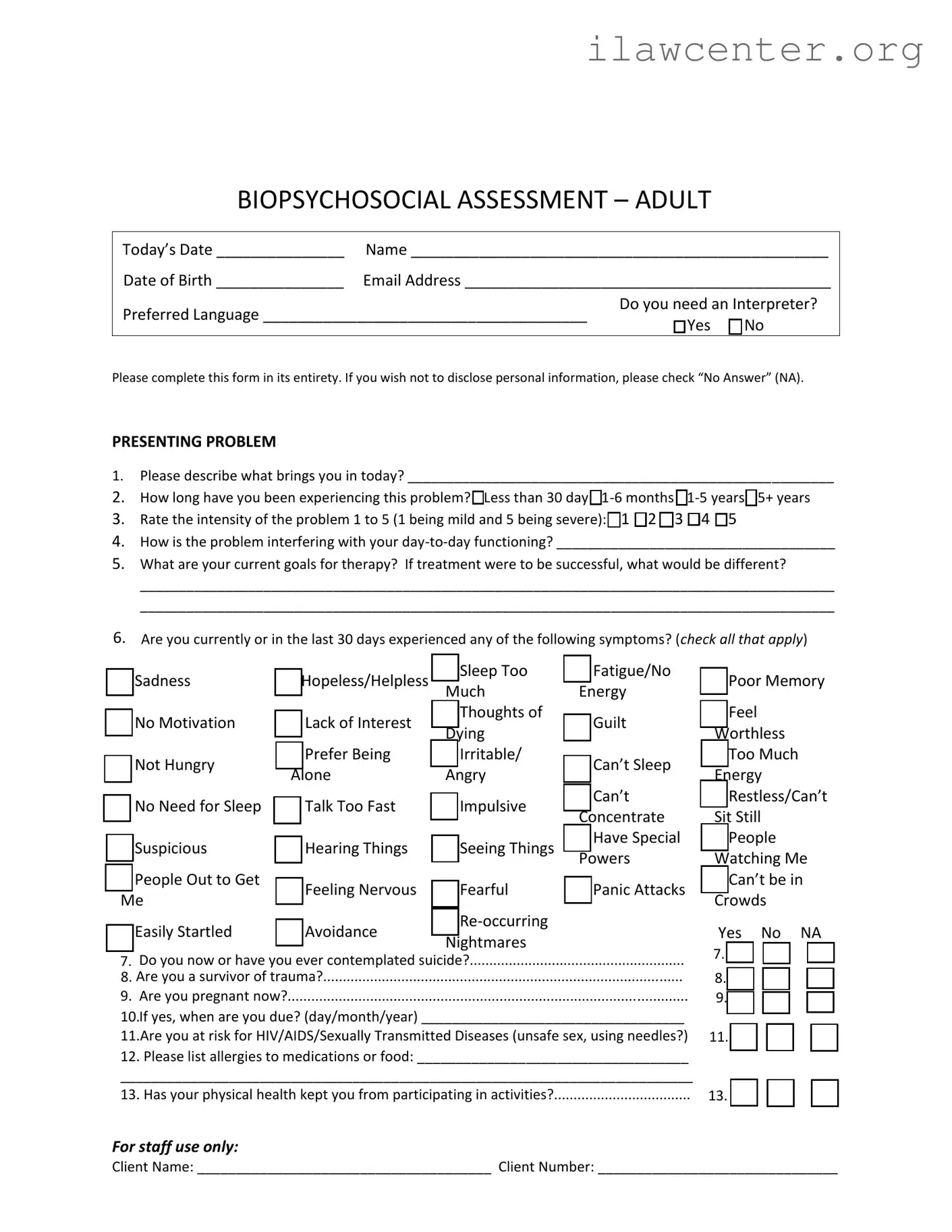
- Begin by entering the today’s date at the top of the form.
- Fill in your name and date of birth accurately.
- Provide your email address and preferred language.
- Indicate if you need an interpreter by checking “Yes” or “No.”
- In the PRESENTING PROBLEM section, describe what brings you in today. Be as detailed as you feel comfortable.
- Indicate how long you have been experiencing this problem by selecting one of the options provided.
- Rate the intensity of the problem on a scale from 1 to 5 by marking the appropriate box.
- Explain how the problem is affecting your day-to-day functioning.
- Outline your current goals for therapy, describing what would be different if treatment were successful.
- Check any symptoms you have experienced in the last 30 days from the list provided.
- Answer the questions regarding suicidal thoughts, trauma, pregnancy, and risk for HIV/AIDS or STDs.
- List any allergies to medications or food.
- Indicate whether your physical health has affected your participation in activities.
- For the TOBACCO section, answer the questions about tobacco use and provide details if applicable.
- In the SUBSTANCE USE/ADDICTION section, respond to the questions regarding current and past substance use issues.
- Describe your personal, family, and relationships situation, including any significant changes in the past 90 days.
- Indicate your marital status and provide details about any relationship issues you may have faced.
- Complete the EDUCATION section by indicating your highest level of education and your school experience.
- In the LEGAL section, respond to questions about any past arrests and legal representation.
- For the WORK section, describe your work history and whether you have served in the military.
- Finally, fill out the MEDICAL section, providing information about your primary care physician, any medical issues, medications, and mental health professionals you have seen.