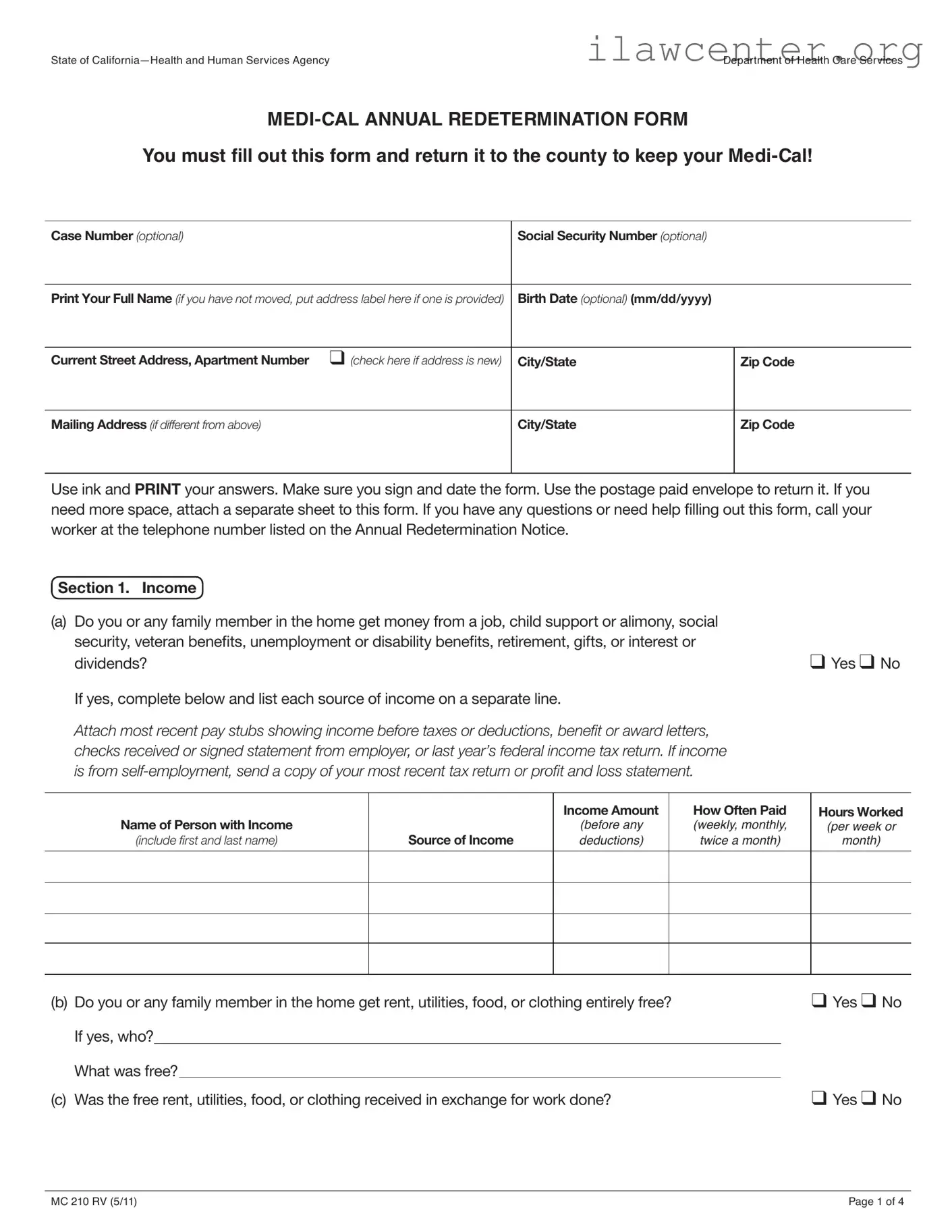
Instructions on Utilizing Medi Cal Redetermination
Completing the Medi-Cal Redetermination form is a crucial step in maintaining your eligibility for Medi-Cal benefits. Once you have filled out the form accurately, it must be returned to your county office. Be sure to include any required documentation to support your answers.
- Begin by writing your Case Number and Social Security Number at the top of the form (both are optional).
- Print your full name clearly. If your address has not changed, you can place an address label here.
- Fill in your birth date in the format (mm/dd/yyyy).
- Provide your current street address, including apartment number, and check the box if your address is new.
- Complete the city, state, and zip code for your current address.
- If you have a different mailing address, fill that in as well, including the city, state, and zip code.
- Use ink to answer all questions and print your responses clearly.
- Sign and date the form at the bottom, ensuring that you include your daytime or message telephone number and home telephone number, checking the box if it is a new number.
- If you need additional space for any section, attach a separate sheet to the form.
- Return the completed form using the postage-paid envelope provided.
After submitting your form, the county will review your information. If any additional documentation is needed, they will reach out to you. It’s important to keep track of any communication from your county office to ensure your Medi-Cal benefits remain uninterrupted.