73115 (10/17)
Release of Protected
Health Information
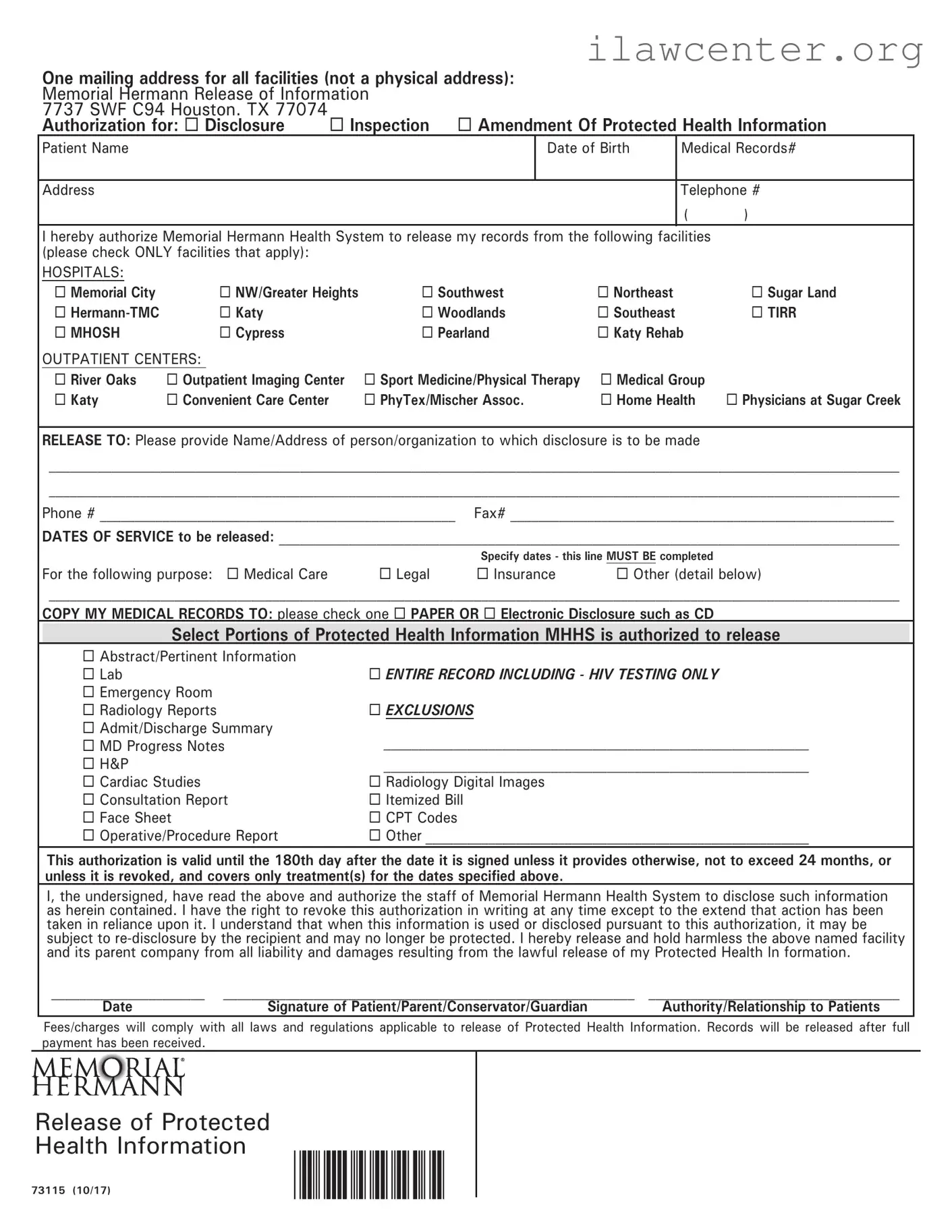
One mailing address for all facilities (not a physical address):
Memorial Hermann Release of Information
7737 SWF C94 Houston. TX 77074
Authorization for: Disclosure Inspection Amendment Of Protected Health Information
Patient Name Date of Birth Medical Records#
Address Telephone #
( )
I hereby authorize Memorial Hermann Health System to release my records from the following facilities
(please check ONLY facilities that apply):
HOSPITALS:
Memorial City NW/Greater Heights Southwest Northeast Sugar Land
Hermann-TMC Katy Woodlands Southeast TIRR
MHOSH Cypress Pearland Katy Rehab
OUTPATIENT CENTERS:
River Oaks Outpatient Imaging Center Sport Medicine/Physical Therapy Medical Group
Katy Convenient Care Center PhyTex/Mischer Assoc. Home Health Physicians at Sugar Creek
RELEASE TO: Please provide Name/Address of person/organization to which disclosure is to be made
__________________________________________________________________________________________________________________________
__________________________________________________________________________________________________________________________
Phone # ___________________________________________________ Fax# _______________________________________________________
DATES OF SERVICE to be released: _________________________________________________________________________________________
Specify dates - this line MUST BE completed
For the following purpose: Medical Care Legal Insurance Other (detail below)
__________________________________________________________________________________________________________________________
COPY MY MEDICAL RECORDS TO: please check one PAPER OR Electronic Disclosure such as CD
Select Portions of Protected Health Information MHHS is authorized to release
Abstract/Pertinent Information
Lab ENTIRE RECORD INCLUDING - HIV TESTING ONLY
Emergency Room
Radiology Reports EXCLUSIONS
Admit/Discharge Summary
MD Progress Notes
_____________________________________________________________
H&P _____________________________________________________________
Cardiac Studies Radiology Digital Images
Consultation Report Itemized Bill
Face Sheet CPT Codes
Operative/Procedure Report Other _______________________________________________________
This authorization is valid until the 180th day after the date it is signed unless it provides otherwise, not to exceed 24 months, or
unless it is revoked, and covers only treatment(s) for the dates specied above.
I, the undersigned, have read the above and authorize the staff of Memorial Hermann Health System to disclose such information
as herein contained. I have the right to revoke this authorization in writing at any time except to the extend that action has been
taken in reliance upon it. I understand that when this information is used or disclosed pursuant to this authorization, it may be
subject to re-disclosure by the recipient and may no longer be protected. I hereby release and hold harmless the above named facility
and its parent company from all liability and damages resulting from the lawful release of my Protected Health In formation.
______________________ ___________________________________________________________ ____________________________________
Date Signature of Patient/Parent/Conservator/Guardian Authority/Relationship to Patients
Fees/charges will comply with all laws and regulations applicable to release of Protected Health Information. Records will be released after full
payment has been received.