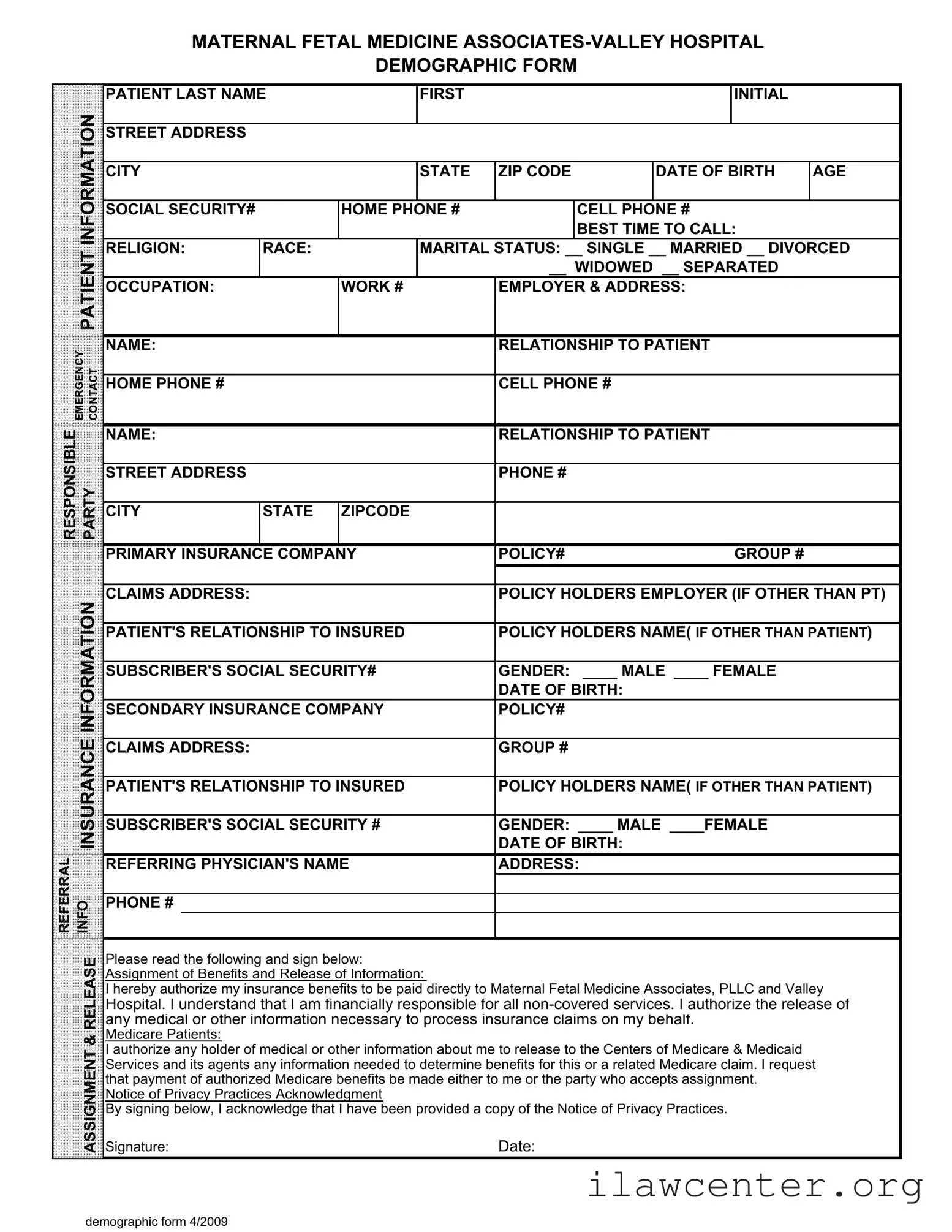
Instructions on Utilizing Patient Demographics
Completing the Patient Demographics form is an important step in ensuring that your medical information is accurately recorded. This information will be used to facilitate your care and communicate with your insurance providers. Follow the steps below to fill out the form correctly.
- Begin with your last name and first initial in the designated fields.
- Provide your street address, city, state, and ZIP code.
- Enter your date of birth and age.
- Fill in your social security number.
- List your home phone number and cell phone number.
- Indicate the best time to call you.
- Provide your religion and race.
- Select your marital status by checking the appropriate box: Single, Married, Divorced, Widowed, or Separated.
- State your occupation and provide your work number and employer's address.
- Fill in the emergency contact name, their relationship to you, and their home and cell phone numbers.
- Provide the responsible party's name and their relationship to you, along with their street address and phone number.
- List your primary insurance company, policy number, and group number.
- Fill in the claims address for your primary insurance.
- Provide the policy holder's employer if it is different from yours.
- Indicate your relationship to the insured if the policy holder is not you.
- Fill in the policy holder's name if it is not you and their social security number.
- Indicate your gender by checking the appropriate box: Male or Female.
- Provide the date of birth for the policy holder.
- Complete the information for your secondary insurance company, including policy number, claims address, and group number.
- Repeat the steps for the secondary insurance regarding policy holder's name and social security number.
- Fill in the referring physician's name, address, and phone number.
- Read the release section and sign your name along with the date.
- Acknowledge receipt of the Notice of Privacy Practices by signing below the acknowledgment section.