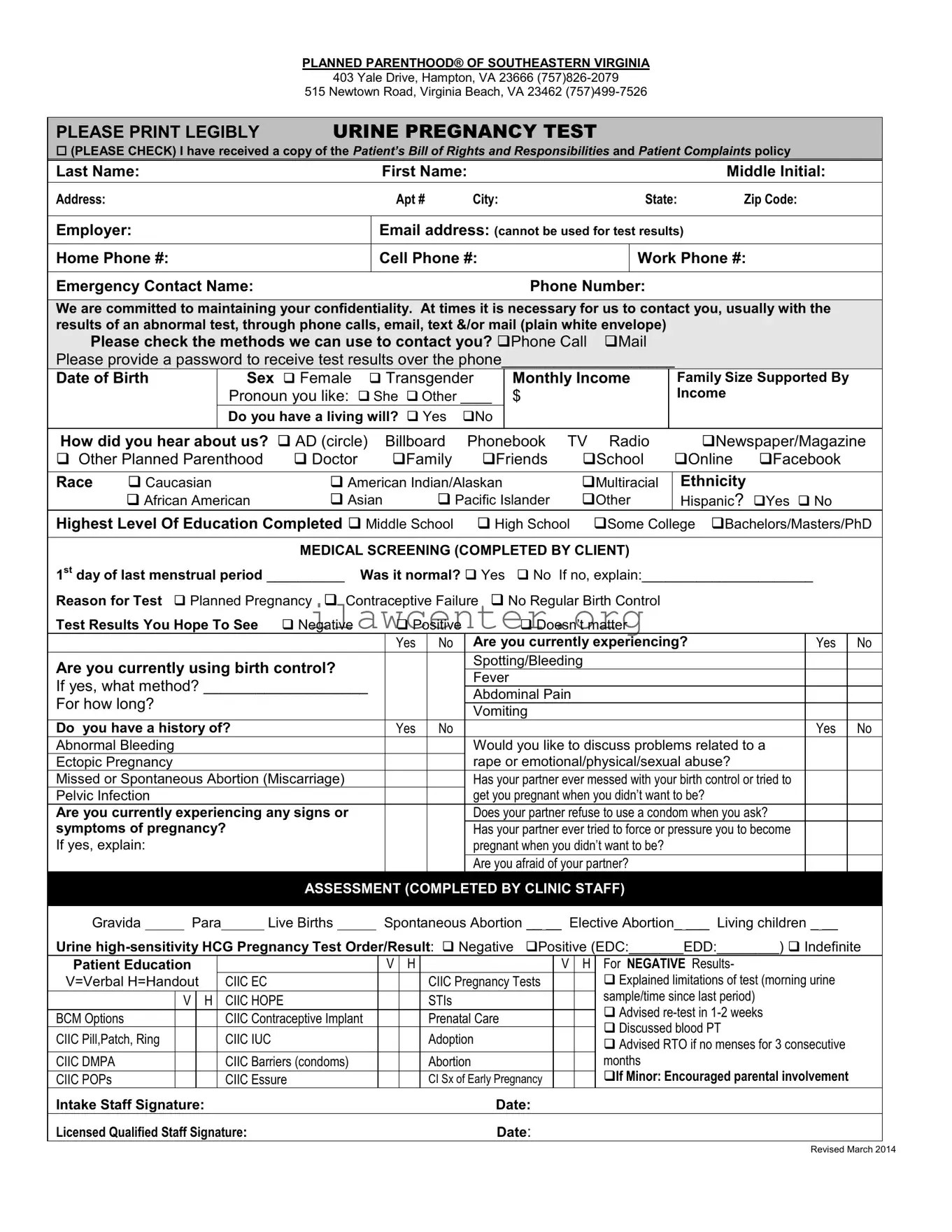
Instructions on Utilizing Planned Parenthood Proof
Filling out the Planned Parenthood Proof form is an important step in receiving the services you need. The form requires personal and medical information to facilitate appropriate care. Below are the steps to complete the form accurately.
- Begin with the section labeled Personal Information. Write your last name, first name, and middle initial.
- Enter your address, including apartment number, city, state, and zip code.
- Fill in your employer's name and email address (note that this email cannot be used for test results).
- Add your home phone number, cell phone number, and work phone number.
- Provide an emergency contact name and phone number.
- Mark how you prefer to be contacted regarding your test results: Phone Call or Mail. Provide a password if you would like to receive results over the phone.
- Indicate your date of birth and sex, and specify your monthly income and family size.
- Choose your preferred pronoun (e.g., She or Other).
- Answer whether you have a living will and how you heard about Planned Parenthood.
- Select your race and whether you identify as Hispanic.
- Specify the highest level of education you have completed.
- In the Medical Screening section, fill in the date of your last menstrual period, and indicate if it was normal.
- State the reason for your test and your desired test results.
- Respond to questions about any current symptoms and whether you are using birth control. If yes, specify the method.
- Provide details about any medical history, particularly regarding pregnancy and birth control issues.
- Complete the section for Assessment if prompted, including information about urine pregnancy tests and any staff evaluations.
- Review the Request for Medical Services section, ensuring you understand the information provided. Sign and date the form as necessary.
Once the form is filled out, you can submit it as per the instructions provided by Planned Parenthood. Remember that staff are available to help with any questions you may have while completing this process.